The Empire Plan is a unique health insurance plan designed especially for public employees in New York State. Empire Plan benefits include inpatient and outpatient hospital coverage, medical/surgical coverage, Centers of Excellence for transplants, infertility and cancer, home care services, equipment and supplies, mental health and substance abuse coverage and prescription drug coverage.

GEORGE E. PATAKI
GOVERNOR
DEPARTMENT OF CIVIL SERVICE
ALBANY, NEW YORK 12239
www.cs.ny.gov
GEORGE C. SINNOTT
COMMISSIONER
DANIEL E. WALL
EXECUTIVE
DEPUTY COMISSIONER
NY04-02
PE04-03
PA04-05
TO: Agency Health Benefits Administrators
FROM: Employee Benefits Division
SUBJECT: National Medical Support Notice Guidelines
DATE: March 26, 2004
This memo will provide you with guidance on the processing of National Medical Support Orders (NMSO) which mandate health insurance coverage for certain children. State and local child welfare agencies began using this form as a result of federal legislation (P.L. 105-200). The NMSO was designed to bring uniformity to the administration of the child medical support orders for both the state social welfare agencies and the employers who receive them. While the requirements of the NMSO are explained in the Employer Response and Administrator Response instructions, this memo contains additional guidance specific to the New York State Health Insurance Program (NYSHIP) to assist you in complying with the NMSO requirements. It is not a substitute for reading the NMSO instructions themselves. A sample NMSO is attached to this memo.
Definitions
Participant: Agency employee and/or NYSHIP enrollee
Employer: Employee's Agency (For NYS agencies the State Comptroller (OSC) is usually listed as the employer on the NMSO but for response activities, the employer is the employee's agency, so OSC forwards the NMSO to you)
Plan Administrator: Employee's Agency
Issuing Agency: The court or Social Services Agency that sends the NMSO to the Employer.
Overview
The Issuing Agency sends the NMSO to the Employer. The order indicates which benefits the child(ren) are required to be enrolled in - usually all available benefits are required: Medical, Dental Vision, Mental Health and Prescription drug. The employee's agency is responsible for enrolling the dependent(s) and/or notifying various stakeholders as described below.
Employer Responsibilities
First determine if the individual identified on the NMSO (participant) is currently your agency's employee and then if they are in a benefits eligible position. If the answer to either of these questions is no, complete the applicable section (2 or 3) of Part A of the NMSO, Employer Response, add your contact information to the bottom of the form and send it to the Issuing Agency.
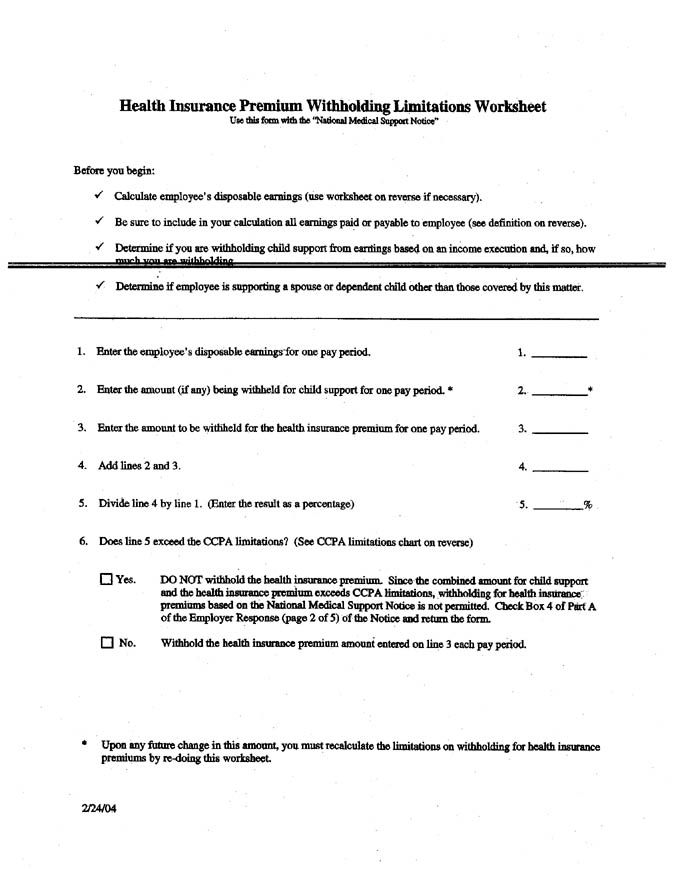
According to NYS law, if health insurance deductions would preclude deductions for full cash child support obligations, the NMSO is not qualified. In this case, check box 4 of Part A of the NMSO, Employer Response, add your contact information to the bottom of the form and send it to the Issuing Agency. If the enrollee has questions regarding withholding limits or prioritization, they should be referred to the Issuing Agency.
If the participant is a current employee of your agency in a benefits eligible position and has wages sufficient to cover the health insurance deduction after cash child support obligations, you do not have to complete the Employer Response and should complete the Administrator Response (Part B of the NMSO).
Administrator Responsibilities
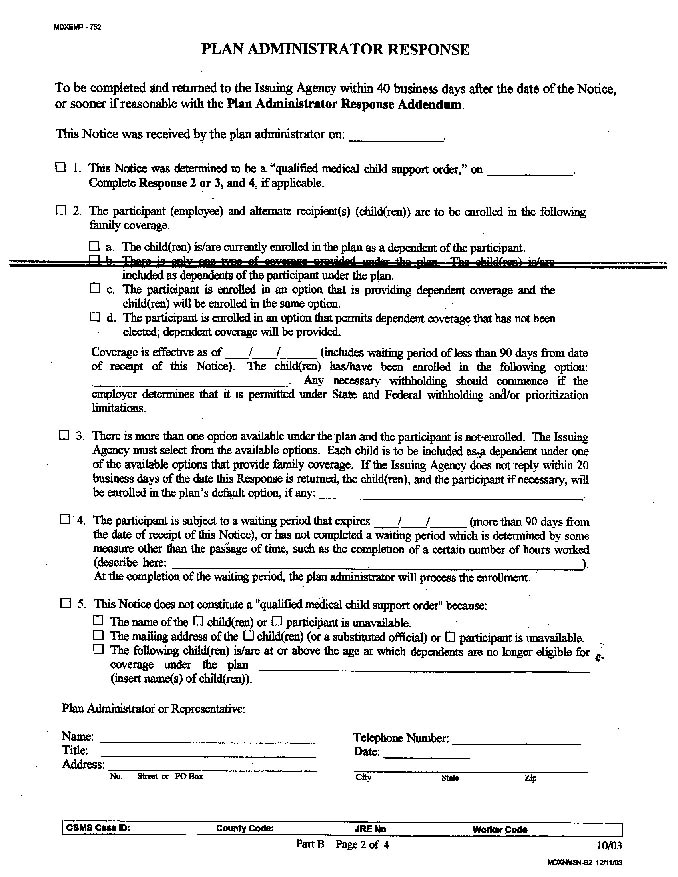
1. Record the date you received the NMSO on Part B, Plan Administrator Response, and determine if the NMSO is qualified. The NMSO is qualified if:
- The participant's name and address are identified or are reasonable accessible; and
- The child(ren)'s name and address(es) or the address of the substituted official or agency are identified or are reasonable accessible; and
- The child(ren) can be covered under NYSHIP*
* The NMSO does not require NYSHIP to provide any benefits to the subject child(ren) which would not be granted to similarly situated dependents. (e.g. dependents over age 19 who are not full time students or disabled under plan definitions are not eligible)
If the NMSO is not qualified, fill out the appropriate section (5) on the Administrator Response and send the NMSO to the Issuing Agency within 40 business days from the date of receipt. If a child is 19 and older (21 and older for Empire Plan subscribers in some negotiating units) indicate in the space provided in section (5) that coverage until age 25 is available upon proof that the child is a full-time student at an accredited secondary school or college.
If the NMSO is qualified, record the date you determined this in section (1) on the Administrator Response and determine the appropriate NYSHIP coverage for the child(ren).
2. Determination of appropriate NYSHIP coverage for the child(ren) will vary based on the enrollee's NYSHIP enrollment circumstances (see below chart). In each case however, the child(ren) should be enrolled with the custodial parent's address, substitute official's address or the substitute agency's address, as indicated on the NMSO. In addition, a health insurance identification card must be issued for the dependent to ensure the dependent can access benefits. Empire ID cards will automatically be sent to newly enrolled Empire Plan dependents. A duplicate card should be requested for currently enrolled Empire Plan dependents. Dependents enrolled in NYSHIP HMOs will get a health insurance identification card and benefit information through one of the notification letters described below.
|
NYSHIP Enrollment circumstance
|
Appropriate NMSO action
|
|---|---|
| Enrollee and dependent(s) currently enrolled | Check the boxes in section 2 a. Fill in the effective date and plan name. |
| Enrollee has family coverage, child(ren) is/are not enrolled | Check the boxes in section 2 c. Enroll the child(ren) effective the first day of the pay period following receipt of the NMSO with a DEP/ADD transaction. Fill in the effective date and plan name. |
| Enrollee has individual coverage | Check the boxes in section 2 d. Change the coverage to family coverage and enroll the child(ren) effective the first day of the pay period following receipt of the NMSO with a CCO/DEP transaction. Fill in the effective date and plan name. |
| Enrollee is eligible but not enrolled | Call the Issuing Agency contact if a number is provided on the NMSO and explain eligible benefit plans. If there is no contact number available, Check box 3, list the Empire Plan as the default plan and forward a Choices guide and rate sheet to the Issuing Agency* |
| Employee has not satisfied the new enrollee waiting period | Check the box in section 4. Indicate that coverage may be available after the waiting period is satisfied. |
* The NMSO requires the Issuing Agency to choose the plan when an eligible participant has more than one option available. In most cases, the Issuing Agency will not reply within 20 days of mailing the Choices guide and rate sheet and you will enroll the employee and child(ren) in the default - Empire Plan family coverage. It has been our experience that if you call the Issuing Agency, and speak to the case worker for the subject of the order and explain that the Empire Plan is both the most popular plan and the only plan that offers nation-wide coverage, then they will invariably choose the Empire Plan. Calling may save you the steps of sending out the choices guide and waiting for Issuing Agency's response.
Note to Participating Agencies: When an Enrollee is eligible but not enrolled, contacting the Issuing Agency is not necessary if your agency only offers the Empire Plan to employees. Check the box in section 2 and enroll the employee and child(ren) in the Empire Plan effective the first day of the pay period following receipt of the NMSO. Fill in the effective date and plan name.
After you have determined the appropriate NYSHIP coverage based on the above chart, fill in your contact information on the bottom of the Administrator Response and notify the stakeholders as described below.
3. Notification Requirements
Boxed areas on the sample letters are included to assist you and should not be included in final notification letters you develop at your agency.
NYBEAS
The NMSO requires that coverage for the dependent under the order can not be cancelled arbitrarily, even at the enrollee's request. A NYBEAS comment should be added reflecting the dependent name, person#, effective date of coverage and that dependent coverage can not be cancelled unless the enrollee or dependent loses eligibility under plan rules, the dependent receives equivalent coverage under another plan or the court order ceases.
Enrollee
See the attached Enrollee Notification Letter sample for assistance in developing your enrollee responses. If enrollees have questions regarding the NMSO refer them to the Issuing Agency.
Custodial Parent
See the attached notification letters to the Custodial Parent for assistance in developing your responses. There is one sample letter confirming the child was previously enrolled and another confirming the child has recently been enrolled in compliance with the NMSO. In either case, copies of the General Information Booklet and Empire Plan Certificate, Empire Plan update reports and HIPAA policy information should be enclosed for Empire Plan dependents. The General Information Booklet for NYHSIP approved Health Maintenance Organizations, HMO update reports and HIPAA policy information should be enclosed for HMO dependents.
Health Insurance Carriers
See the attached Carrier notification letters for assistance in developing your responses. Empire Plan carriers are told that we have updated our enrollment file in compliance with the NMSO and to process claims for the unemancipated dependents. HMOs are similarly notified but additionally asked to provide health insurance identification cards and benefit information to the dependents.
Issuing Agency
See the attached Issuing Agency notification letters for assistance in developing your responses. One sample is a simple cover letter to the NMSO supplied as proof of compliance with the order.
Note to NYS Agencies: Another sample letter is used to notify the Issuing Agency that a Union Benefit Fund should be contacted as the Plan Administrator for dental and/or vision benefits. This would apply to employees represented by the Civil Service Employee Association, United University Professions or District Council 37.
The Issuing Agency should also be notified if the participant terminates the employment relationship with your agency.
Questions concerning the processing of the NMSO may be forwarded to your agency processor.
For a paper copy of these materials, contact your processor in the Employee Benefits Division of the NYS Department of Civil Service.
Sample Envelope and Enclosure List
Part A - Notice to Withhold for Health Care 1 | 2 | 3 | 4 | 5
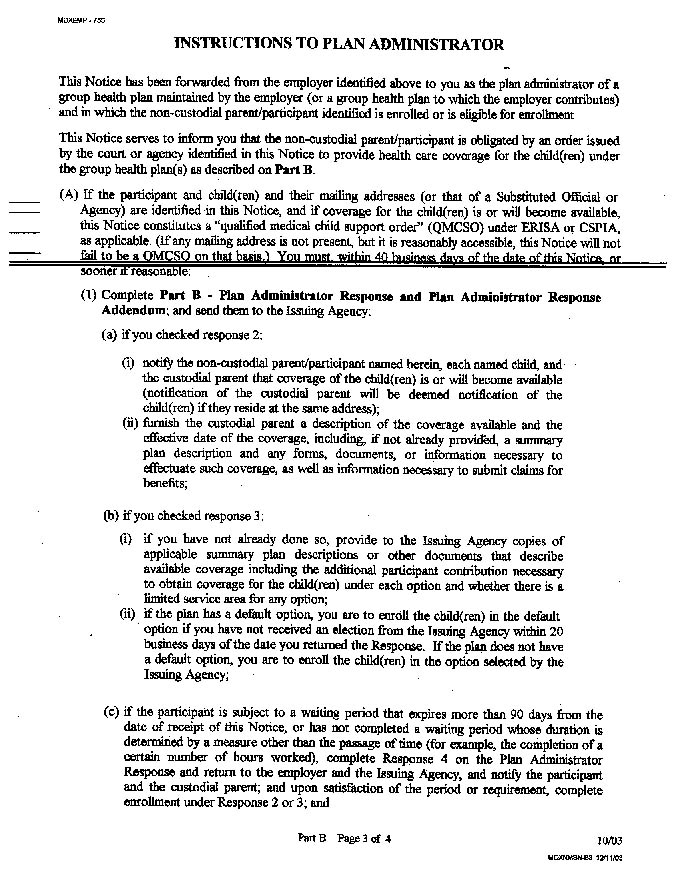
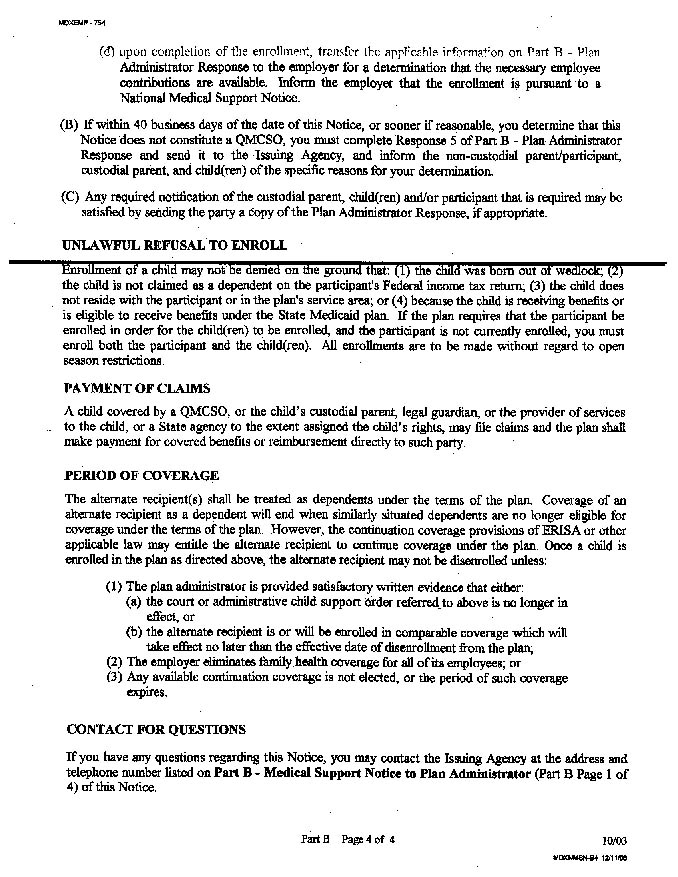
Part B - Medical Support Notice to Plan Administrator 1 | 2 | 3 | 4
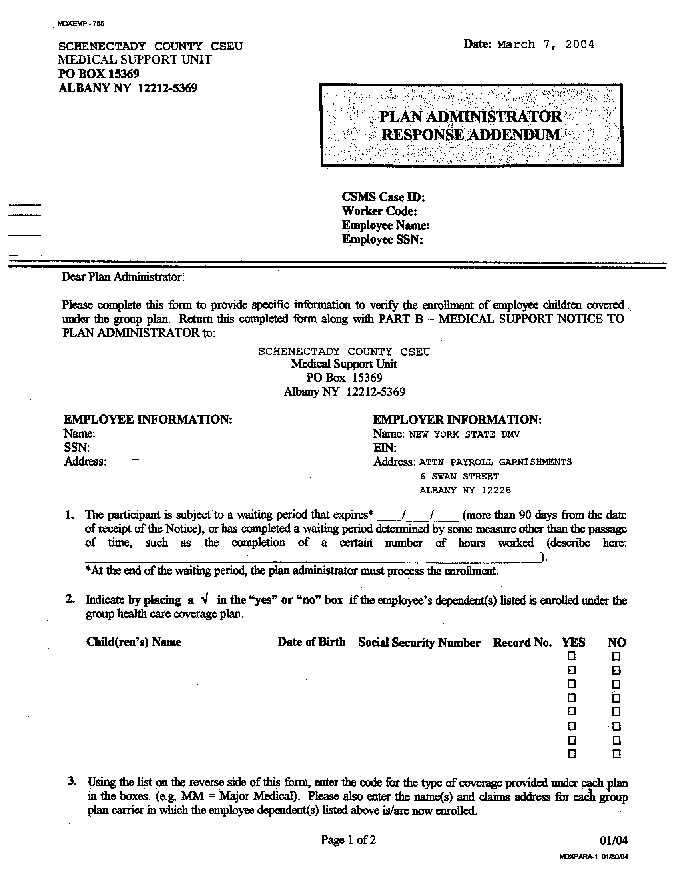
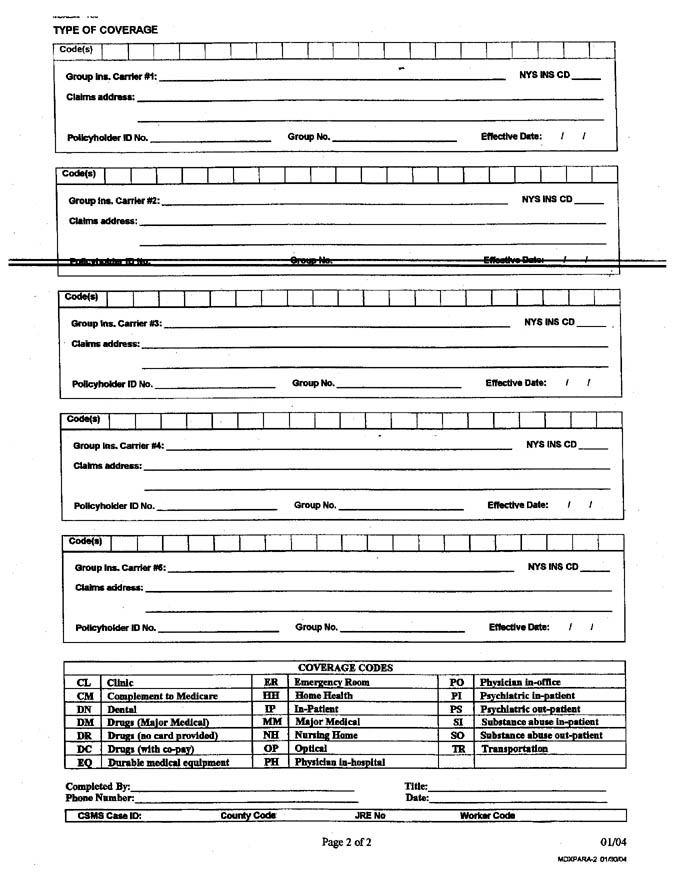
Plan Administrator Response Addendum 1 | 2
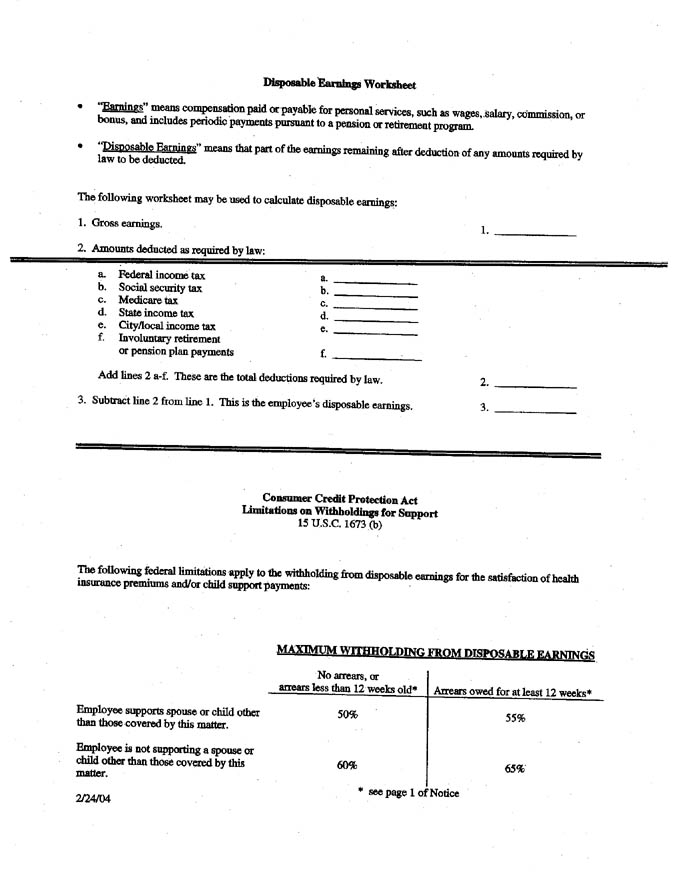
Health Insurance Premium Withholding Limitations Worksheet
Disposable Earnings Worksheet
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Empire Carrier Notification
Date
Empire Carrier Name
Empire Carrier Street Address
Empire Carrier City/State/Zip
RE: (Enrollee Name)
SS # (Enrollee SS#)
Dear Empire Carrier Name:
Enclosed is a copy of a National Medical Support Notice (Notice) for (Enrollee's Name). Please process claims for the dependent(s) in accordance with the terms of the Notice.
Thank you for your cooperation.
Sincerely,
HBA Name
HBA Title
Enclosure
Note: Each Empire Plan Carrier must be sent a copy of the National Medical Support Notice. The carrier addresses may be found in the General Information Booklet.
Health Maintenance Organization Notification
Date
HMO Name
HMO Street Address
HMO City/State/Zip
RE: (Enrollee Name)
SS # (Enrollee SS#)
Dear HMO Name:
Enclosed is a copy of a National Medical Support Notice (Notice) for (Enrollee's Name). Please update your records and process claims for the dependent(s) in accordance with the terms of the Notice. In addition, please send cards and any necessary benefit information to the appropriate address (custodial parent address or substitute official address) on the Notice.
Thank you for your cooperation.
Sincerely,
HBA Name
HBA Title
Enclosure
Note: The HMO addresses may be found in the Choices guide
Issuing Agency Notification
Date
Issuing Agency Name
Issuing Agency Street Address
Issuing Agency City/State/Zip
RE: (Case #)
To Whom It May Concern:
Enclosed is the Plan Administrator Response to the National Medical Support Notice for (Enrollee's name), SS# (Enrollee's SS#).
Sincerely,
HBA Name
HBA Title
Enclosure
Issuing Agency - EBF Notification
Date
Issuing Agency Name
Issuing Agency Street Address
Issuing Agency City/State/Zip
RE: (Case #)
To Whom It May Concern:
Enclosed is the Plan Administrator Response to the National Medical Support Notice for (Enrollee's name), SS# (Enrollee's SS#).
Please be advised that the enrollee has health insurance through the New York State Health Insurance Program (NYSHIP). However, the dental and vision coverage is provided through the (Union Benefit Fund Name). You may contact them at (Union Benefit Fund telephone number) or by writing to:
(Union Name) Benefit Fund
(Street Address)
(City/State/Zip)
Sincerely,
HBA Name
HBA Title
Enclosure
Union Benefit Fund Contact Information
CSEA Employee Benefit Fund
1 Lear Jet Lane Suite 1
Latham, NY 12110-2395
800 323-2732
United University Professions
Benefit Trust Fund
800 Troy-Schenectady Road
Latham, NY 12110-2455
800-887-3863
District Council 37
AFSCME, AFL-CIO
125 Barclay Street
New York, NY 10007
(212) 815-1000
Custodial Parent Notification
Adding dependent(s)
Date
Custodial Parent Name
Custodial Parent Street Address
Custodial Parent City/State/Zip
RE: (Case #)
Dear Custodial Parent Name:
This concerns the National Medical Support Notice for [name of dependent(s)]. Pursuant to the notice, we are confirming enrollment as a dependent of [enrollee's name] effective [date of coverage] in the following plans in the New York State Health Insurance Program:
Health Insurance Empire Plan or HMO
Dental Coverage GHI Dental Plan
Vision Coverage Davis Vision
Only list health insurance if dental and vision benefits are administered through a union benefit fund
Please be advised, we have updated the dependent's address(es) as above. We have requested new health insurance card(s) to go to the above address. In addition, we have enclosed useful materials describing plan benefits and eligibility rules for Empire Plan dependents or have requested similar materials be sent to you from an HMO if applicable. Enrollment questions should be directed to our office at [HBA telephone].
Sincerely,
HBA Name
HBA Title
Enclosure
Note: Enclosures include: a copy of the NMSO, and a General Information Booklet and addendums for the Empire Plan or HMOs as applicable.
Custodial Parent Notification
Confirming dependent(s) currently enrolled
Date
Custodial Parent Name
Custodial Parent Street Address
Custodial Parent City/State/Zip
RE: (Case #)
Dear Custodial Parent Name:
This concerns the National Medical Support Notice for [name of dependent(s)]. Pursuant to the notice, we are confirming that the above noted child(ren) are already enrolled as [a] dependent[s] of [enrollee's name] in the following plans in the New York State Health Insurance Program:
Health Insurance: Empire Plan or HMO
Dental Coverage: GHI Dental Plan
Vision Coverage: Davis Vision
Only list health insurance if dental and vision benefits are administered through a union benefit fund
Please be advised, we have updated the dependent's address(es) as above. We have requested new health insurance card(s) to go to the above address. In addition, we have enclosed useful materials describing plan benefits and eligibility rules for Empire Plan dependents or have requested similar materials be sent to you from an HMO if applicable. Enrollment questions should be directed to our office at [HBA telephone].
Sincerely,
HBA Name
HBA Title
Enclosure
Note: Enclosures include: a copy of the NMSO, and a General Information Booklet and addendums for the Empire Plan or HMOs as applicable.
Enrollee Notification
Date
Enrollee Name
Enrollee Street Address
Enrollee City/State/Zip
RE: (Case #)
Dear Enrollee Name:
This concerns the National Medical Support Notice for [name of dependent(s)]. Pursuant to the notice, we are confirming enrollment as your dependent effective [date of coverage] in the following plans in the New York State Health Insurance Program:
Health Insurance: Empire Plan or HMO
Dental Coverage: GHI Dental Plan
Vision Coverage: Davis Vision
Only list health insurance if dental and vision benefits are administered through a union benefit fund
Please be advised, we have updated the dependent's address(es) to reflect that of the custodial parent. Any question regarding this issue may be directed to our office at [HBA telephone].
Sincerely,
HBA Name
HBA Title
Enclosure
Note: Enclosure a copy of the NMSO. The second sentence applies to an enrollee that currently has individual coverage. You will have to modify this sentence to cover enrollees with various enrollment situations such as those with existing family coverage or enrollees that are not currently enrolled in any health insurance plan.